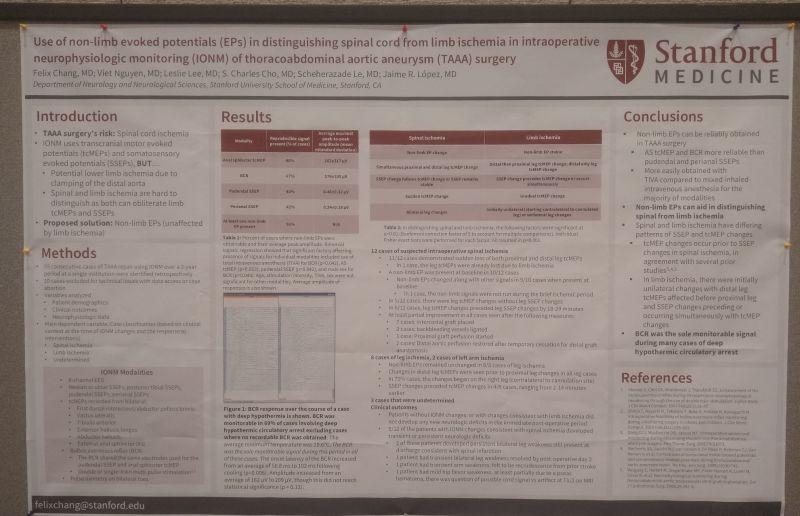
I thought this was a clever addition to traditional #ionm for TAAA surgery.
Using a non-limb modality (BCR, anal tcMEP, pudendal, and anal EP) the authors looked to better differentiate spine from limb ischemia.
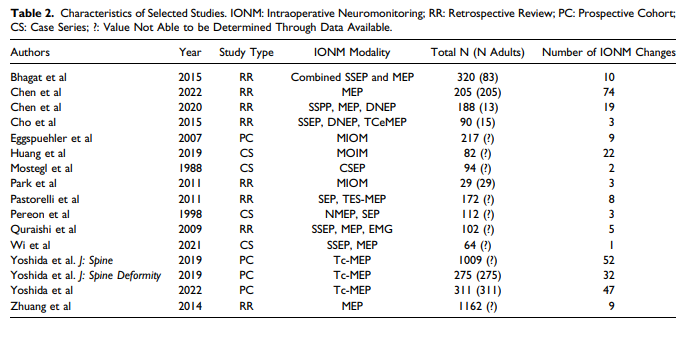
A small sample size, but you can see the low rate of establishing BSL is improved when trying them all.
You get what you get, but better than nothing.
And talk about a great experience for newcomers to the field clinicians looking to learn different modalities.